The counters and furniture should be tough to withstand a lot of heavy use. Easy to clean and maintain
· Connections should be made of metal—to—metal fasteners
· Cabinet-quality wood construction should also be tough and strong
· Surfaces for counters should be solid, non-porous and stain resistant
· Fabrics should be durable, colourfast and flame and static resistant if possible
· Bedside clocks, calendars and bulletin boards help the conscious patient well oriented and in better moods
· Providing the patient with a place to keep a few small personal items of their own make the environment more familiar and personalized.
· Some finishing touches like some art work/décor/ sculpture may change the ICU atmosphere a great deal and has been recommended by the SCCM.
· Chairs number and types
· Individual units should decide about the number, usually enough number to accommodate the care giving staff/doctors and Nurses and additional chairs may be stored and used whenever needed.
· Individual Units should decide whether they want to allow the relative to sit by the side (Short or long time) of the patient in the ICU.
· However, a chair/sofa type chair on wheels with safety belt or vault is recommended for mobilising the patient. and making him sit during recovery
· Provisions must be made to accommodate an obese patient
FLOOR, WALL AND CEILING COVERINGS
Floor –
· The ideal floor should be easy to clean, non slippery, able to withstand abuse and absorb sound while enhancing the overall look and feel of the environment
· Carts and beds equipped with large wheels should roll easily over it. In Indian context Vitrified non-slippery tiles seem to be the best option which can be fitted into reasonable budgets, easy to clean and move on and may be stain proof
· Vinyl sheeting is another viable option, It can be non-porous, strong and easy to clean, However, the life of Vinyl flooring is not long and a small damage in one corner may trigger damage of entire flooring and make it accident prone. It may require frequent replacement making it to be inconvenient choice.
Walls – Should meet following criteria:
· Durability, ability to clean and maintain, flame retardance, mildew resistance, sound absorption and visual appeal.
· It has been very useful to have a height up to 4to5 ft finished with similar tiles as of floor for similar reasons. 17
· For rest of the wall soothing paint with glass panels on the head end at the top may be good choice.
· Wooden panelling has also found favour with some architects but costs may go high.
· Doorstoppers and handrails should be placed well to reduce abuse and noise to minimum; it helps patient movement and ambulation.
Ceiling

· lt is the ceiling surface patients see most often, sometimes for hours on end, Over several days or weeks, In addition, bright spotlights or fluorescent lights can cause eye strain,
· Ceiling should be Soiling and break proof due to leaks and condensation.
· Tiles may not the most appealing or soothing surface, but for all practical purposes it is easier to remove individual or few tiles for repairs over ceiling in times of need. Ceiling design may be enhanced by varying the ceiling height, softening the contours, griddled lighting surfaces, painting it with a medley of soft colours rather than a plain back ground colour, or decorating it with mobiles, patterns or murals, to make it more patient and staff friendly.
· It is recommended that no lines or wires be kept or run over ceiling or underground because damages do occur once in a while and therefore, it should be easy to do repairs if the lines and pipes are easily explorable without hindering patient care
Waste Disposal and Pollution Control
· This is mandatory and a huge safety issue both for the patient and staff/doctors of the hospital and society at large
· It is important that all govt regulations (State Pollution control Board in this particular case) should strictly be complied with.
· It is mandatory to have four covered pans (Yellow, blue, Red, Black) provided for each patient or may be one set between two patients two save space and funds. This is needed to dispose off different grades of wastes.

Hand Hygiene and Prevention of Infection
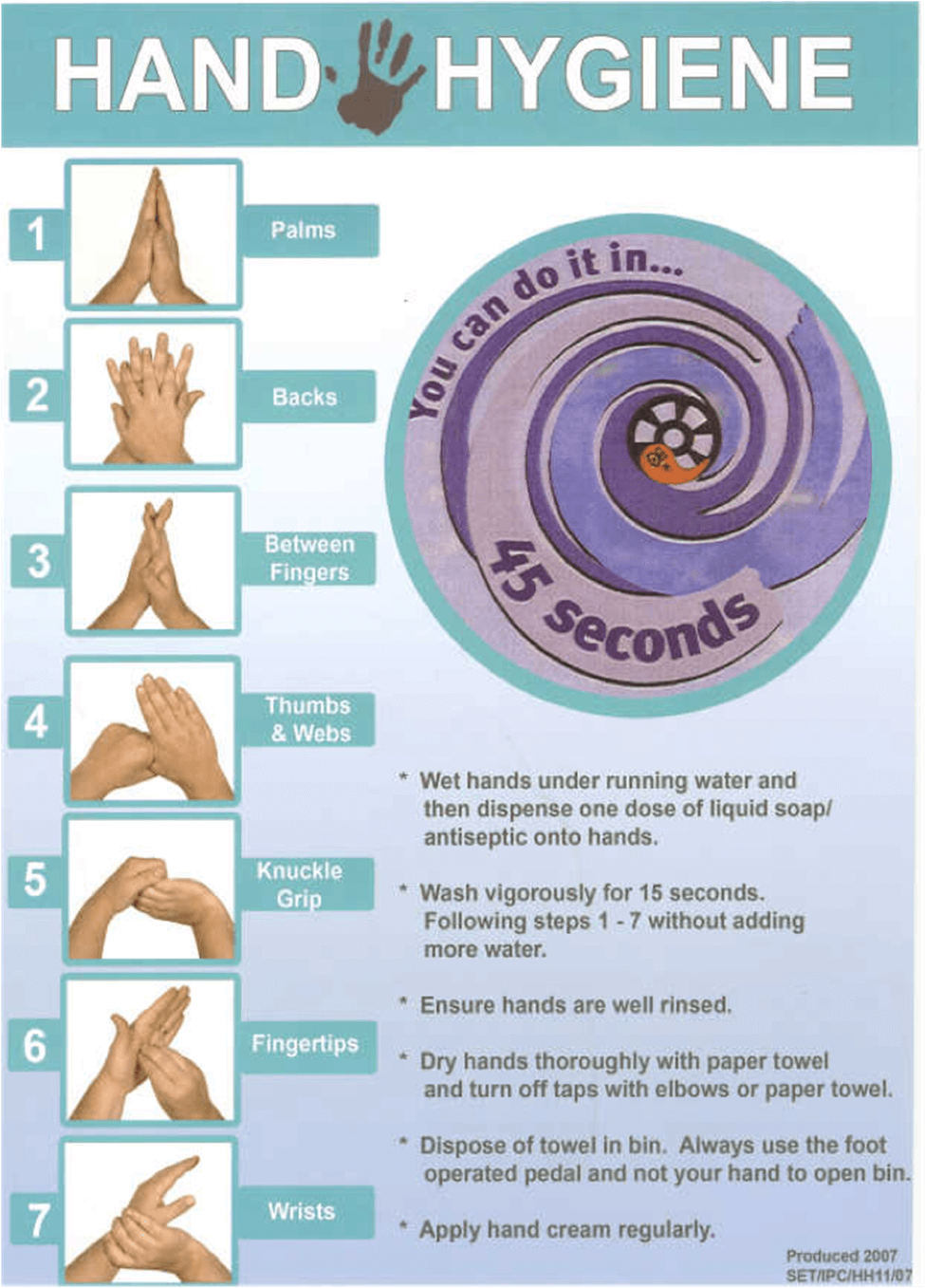
· Every bed should have attached alcohol based anti-microbial instant hand wash solution source, which is used before caregiver (doctor/Nurse/relative/Paramedical) handles the patient.
· Water basin at all bedside has not proven popular and successful because of poor compliance by one and all and also for reasons of space constraints and maintenance issues.
· An operation room style sink with Elbow or foot operated water supply system with running hot and cold water supply with antiseptic soap solution source should be there at a point easily accessible and unavoidable point, where two people can wash hands at a time.
· This sink should have an immaculate drainage system, which usually may become a point of great irritation and nuisance in later yrs or months.
· All entrants (Irrespective of Doctors or nurses should don mask and cap in ICU and ideally an apron which should be replaced daily)
· No dirty/soiled linen/material should be allowed to stay in ICU for long times for fear of spread of bad odour, infection and should be disposed off as fast as possible.
· Dirty linen should be replace regularly at fixed intervals.